Basic Knee Anatomy
INTRODUCTION TO THE KNEE
The knee is the largest joint in the body, and with that, the knee is also one of the most complex. There are several different parts of the knee which allow it to have a range of movement. This allows humans to preform many different tasks, such as walking, jumping, and running. As it is very complex, the knee is also more susceptible to injury than other parts of the body. MedicalNewsToday even says, "The knee is the most commonly injured joint by adolescent athletes with an estimated 2.5 million sports-related injuries yearly". Understanding the basic knee anatomy makes it much easier to comprehend the gravity of knee injuries for athletes, and further, why females are more susceptible to injury than males.
ANATOMY
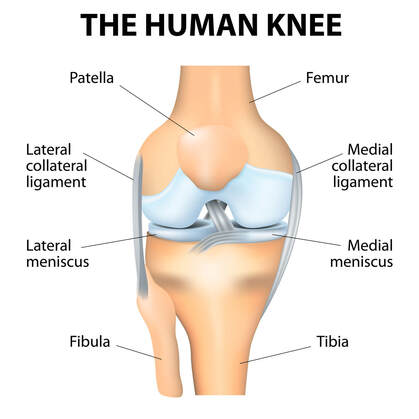
Most basically, the knee connects the femur (thigh bone) to the tibia (shin bone), and is protected by the patella (knee cap). The knee is a joint, which means it is a point where two bones meet. More specifically, the knee is a synovial joint. A synovial joint is a joint cavity filled with fluid, which provides a wide range of motion to the knee, and also keeps the joint lubricated. There are two different types of cartilage in the knee. Cartilage is a connective tissue in the body, that is tough but flexible. The two types of cartilage in the knee are the meniscus and the articular cartilage. The meniscus consists of two semicircle pieces of rubbery cartilage that are located on the inner (medial) and outer (lateral) sides of the knee. The meniscus helps to cushion the knee, and protect the bones from rubbing against each other, and also to improve balance and stability. The other type of cartilage in the knee is called articular cartilage. Articular cartilage is a thin, white, slippery cartilage that is found on the end of bones – on the femur, the top of the tibia, and the back of the patella. Articular cartilage is a very important part of the knee structure because it allows the bones to move across each other, as well as serves as a shock absorber. Another pivotal part of the knee anatomy are the ligaments. The ligaments connect the bones to one another. There are four ligaments in the knee, two that are collateral (on the sides of knee) and two that are cruciate (on center of knee):
The knee is the largest joint in the body, and with that, the knee is also one of the most complex. There are several different parts of the knee which allow it to have a range of movement. This allows humans to preform many different tasks, such as walking, jumping, and running. As it is very complex, the knee is also more susceptible to injury than other parts of the body. MedicalNewsToday even says, "The knee is the most commonly injured joint by adolescent athletes with an estimated 2.5 million sports-related injuries yearly". Understanding the basic knee anatomy makes it much easier to comprehend the gravity of knee injuries for athletes, and further, why females are more susceptible to injury than males.
ANATOMY
Most basically, the knee connects the femur (thigh bone) to the tibia (shin bone), and is protected by the patella (knee cap). The knee is a joint, which means it is a point where two bones meet. More specifically, the knee is a synovial joint. A synovial joint is a joint cavity filled with fluid, which provides a wide range of motion to the knee, and also keeps the joint lubricated. There are two different types of cartilage in the knee. Cartilage is a connective tissue in the body, that is tough but flexible. The two types of cartilage in the knee are the meniscus and the articular cartilage. The meniscus consists of two semicircle pieces of rubbery cartilage that are located on the inner (medial) and outer (lateral) sides of the knee. The meniscus helps to cushion the knee, and protect the bones from rubbing against each other, and also to improve balance and stability. The other type of cartilage in the knee is called articular cartilage. Articular cartilage is a thin, white, slippery cartilage that is found on the end of bones – on the femur, the top of the tibia, and the back of the patella. Articular cartilage is a very important part of the knee structure because it allows the bones to move across each other, as well as serves as a shock absorber. Another pivotal part of the knee anatomy are the ligaments. The ligaments connect the bones to one another. There are four ligaments in the knee, two that are collateral (on the sides of knee) and two that are cruciate (on center of knee):
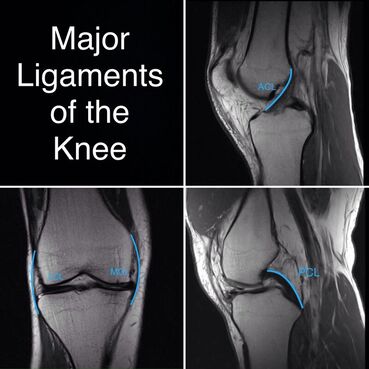
- Anterior cruciate ligament (ACL) - located in the front of the knee, prevents femur and tibia from sliding into one another
- Posterior cruciate ligament (PCL) - located in the back of the knee, also prevents femur and tibia from sliding into one another
- Medial collateral ligament (MCL) - located on the inside of the knee joint, prevents the femur from moving side to side
- Lateral collateral ligament (LCL) - located on the outside of the joint, also prevents side-to-side movement of the femur
The tendons in the knee are also an important part in maintaining its function. The two main tendons in the knee are the patellar tendon and the quadricep tendon. These work to attach muscles to the knee joint. These said muscles are the quadriceps, hamstrings, and gluteal muscles. All provide strength to the knee, as well as allow movement.
Tendons vs Ligaments
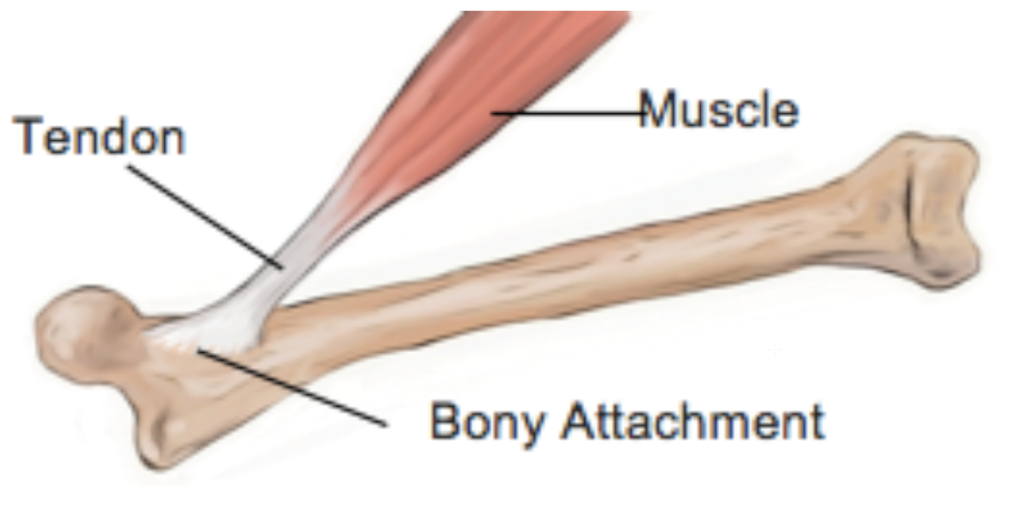
Tendonsattach MUSCLES to BONE
|

Ligamentsattach BONE to BONE
|
The ACL

The ACL, or anterior cruciate ligament, is a piece of tissue that provides rotational stability to the knee. The ACL, also helps hold the bones of the knee together. The ACL connects the thighbone to the shinbone, and runs diagonally across the knee. Along with providing stability to the knee, the ACL also holds the tibia in place, keeping it out of the way of the femur.
ACL tears happen most commonly when an athlete does a sudden change of direction or pivots on a locked knee. The sports that we play – lacrosse and field hockey – involve a lot of sudden stops, as well as change of direction in the form of cutting and dodging. Along with this, ACL tears can also occur from jumping and landing, as well as bumping into another athlete. When the ACL is torn, the athlete can usually hear a sound resembling a "pop". This is usually followed by extreme pain, and quick swelling of the knee.
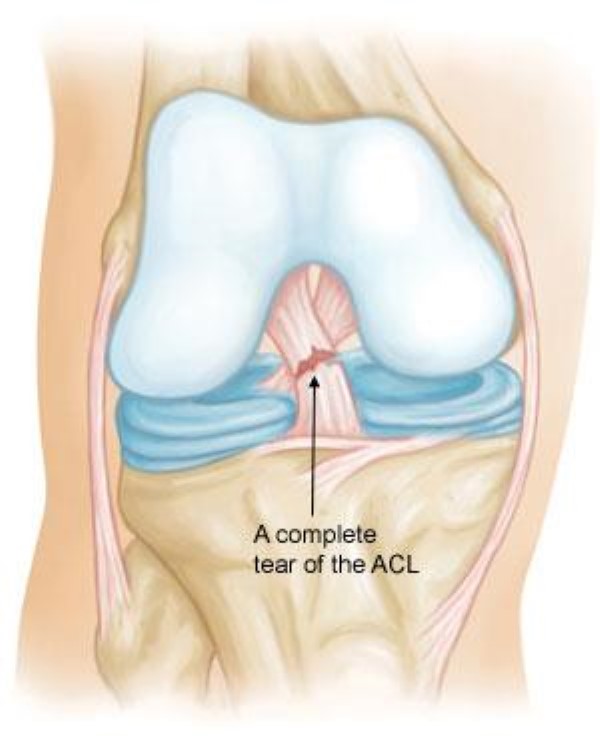
The ACL can be torn in a variety of ways. Once it is torn, there are also multiple severities of the injury, called "grades". A Grade 1 injury is not very severe, and the ligament is just stretched, rather than ripped or torn. Grade 2 injuries result in an ACL that is stretched and partially torn. Grade 3 injuries are the most severe, and result in a complete tear of the ligament. Grade 2 and Grade 3 tears are most commonly treated by surgery, while Grade 1 can be treated without. After surgery, or in lieu of surgery, a knee brace can work to provide stability to the injured leg. Usually, these braces hinder movement so the knee can not bend, or can only bend to a certain degree that is adjusted on the brace
ACL tears happen most commonly when an athlete does a sudden change of direction or pivots on a locked knee. The sports that we play – lacrosse and field hockey – involve a lot of sudden stops, as well as change of direction in the form of cutting and dodging. Along with this, ACL tears can also occur from jumping and landing, as well as bumping into another athlete. When the ACL is torn, the athlete can usually hear a sound resembling a "pop". This is usually followed by extreme pain, and quick swelling of the knee.
The ACL can be torn in a variety of ways. Once it is torn, there are also multiple severities of the injury, called "grades". A Grade 1 injury is not very severe, and the ligament is just stretched, rather than ripped or torn. Grade 2 injuries result in an ACL that is stretched and partially torn. Grade 3 injuries are the most severe, and result in a complete tear of the ligament. Grade 2 and Grade 3 tears are most commonly treated by surgery, while Grade 1 can be treated without. After surgery, or in lieu of surgery, a knee brace can work to provide stability to the injured leg. Usually, these braces hinder movement so the knee can not bend, or can only bend to a certain degree that is adjusted on the brace
Experience & Surgery
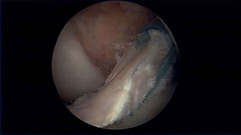
When an ACL is torn, typically there is also meniscal damage. The meniscus is fibrocartilaginous tissue that plays a key factor for a healthy knee joint. The knee joint contains the meniscus, comprised of medial and lateral components. Located between the femur and tibia, the menisci function as shock absorbers or cushions to decrease stress on the knee during weight bearing forces on the knee; such as walking, running, & jumping. When an athlete experiences damage to both the ACL and meniscus, they must be repaired through surgery, which generally lengthens the recovery time.
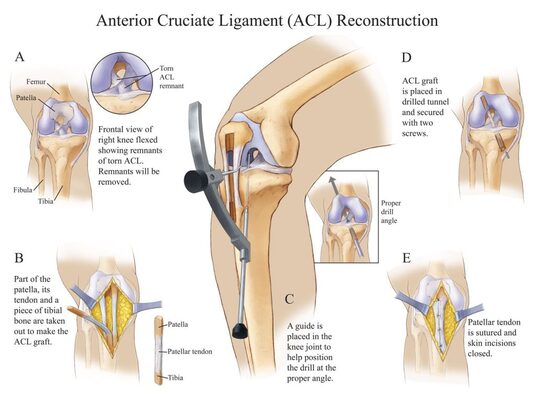
Seen in the image below, are the steps of a typical ACL reconstruction surgery. In this example, a patella tendon graft is used to replace the fully torn Anterior Cruciate Ligament. There are different options your surgeon and Physician Assistant will discuss with the patient to decide which graft is best suited for each individual. The most typical graft used for reconstruction is the Patellar tendon. Since the development of ACL reconstruction surgery, this particular graft has proven the most successful in recovery, especially in younger athletes. The NFL player, Adrian Peterson, who tore his ACL in 2011, used the patellar graft for reconstruction surgery and played in week 1 of the 2012 season only 8 months post-op. A somewhat newer technique, orthopedic surgeons now recommend to high performance athletes is the Quadricep graft. It has been around for some time but has been becoming more popular in the past 5 years. Overall, an individuals body reacts to the graft differently & depending on the patients circumstances one approach may be better than the other.
Seen in the image below, are the steps of a typical ACL reconstruction surgery. In this example, a patella tendon graft is used to replace the fully torn Anterior Cruciate Ligament. There are different options your surgeon and Physician Assistant will discuss with the patient to decide which graft is best suited for each individual. The most typical graft used for reconstruction is the Patellar tendon. Since the development of ACL reconstruction surgery, this particular graft has proven the most successful in recovery, especially in younger athletes. The NFL player, Adrian Peterson, who tore his ACL in 2011, used the patellar graft for reconstruction surgery and played in week 1 of the 2012 season only 8 months post-op. A somewhat newer technique, orthopedic surgeons now recommend to high performance athletes is the Quadricep graft. It has been around for some time but has been becoming more popular in the past 5 years. Overall, an individuals body reacts to the graft differently & depending on the patients circumstances one approach may be better than the other.
Different Grafts/Approaches
The following information was provided by Dr. Mark Sando from the Medical Orthopedic Group of Tampa Bay who is an internationally recognized orthopedic surgeon specializing in sports medicine, arthroscopy and injuries of the shoulder, knee and hip. Info found from his article
ACL RECONSTRUCTION: WHICH GRAFT TYPE IS RIGHT FOR ME? 1/18/21
ACL RECONSTRUCTION: WHICH GRAFT TYPE IS RIGHT FOR ME? 1/18/21

Allograft tendon
This type of graft is the least likely approach a doctor would offer. The allograft tendon means the graft is taken from a cadaver to recreate a ligament in reconstruction surgery. This specific graft is associated with a higher re-tear rate than the other grafts. Probably because the tendon is not as strong as a fresh graft from the patient. Also the graft is least likely to take to the patients body easily. |
|
Quadricep tendon
This autograft is considered the "new kid on the block". The tendon is a thick and robust graft, meaning it has the same reliability of a patellar tendon graft. Benefits:
|
What Does Surgery Entail?
|
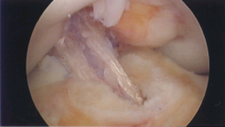
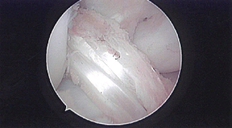
The first step is to remove the damaged anterior cruciate ligament, so the surgeon has room to insert the replacement tendon. Next is to harvest the chosen graft. If it is the patellar tendon autograft, then part of the patella, its tendon and a piece of the tibial bone, are taken for the graft. If it is taken from the hamstring, then 2 of the smaller hamstring muscles -- the gracilis and semitendinosus-- are harvested on the medial side of the knee just below the joint line. Once the surgeon has the graft, they will drill sockets or tunnels into the thighbone and shinbone. This is where the graft will be put, so the tunnel must be drilled at the proper angle through the knee joint. The graft is then secured in the tunnel with two screws or stitches. Once the new ACL is securely in place, all the incisions are closed with stitches.
|
|
Women's Anatomy
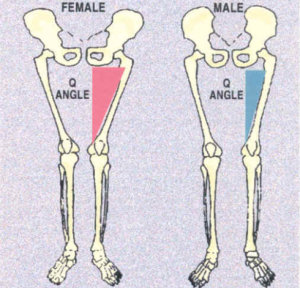
Women are much more susceptible to ACL injury than their male counterparts, even despite playing the same sports at the same rigor. This is because women are anatomically built differently than men, because at the end of the day, their bodies are made to serve different purposes. There are a few different technical and physical differences in men and women that accounts for this disparity in ACL tears:
- Women have a greater elasticity in their ligaments than men, causing them to be more easily stretched and movable. This makes an ACL tear much more likely, since it's more common for the ligament to stretch and twist and eventually tear.
- Women tend to preform more flat-footed landings than men, which causes the knee to absorb more of the shock than the quadricep muscles. This is why in our stretching and exercise program, we focus heavily on practicing safe jumping and landing techniques.
- Women have a lesser core stability than men. The core controls the overall motion and control of the body. With a less stable core, women have overall less movement control, leading to more injury.
- The difference in neuromuscular activation patterns is another factor that contributes to the increased amounts of ACL tears in women. Women are less effective in stiffening their knee, as well as having less muscle strength and endurance. The strength and endurance of the muscles surrounding the knee is pivotal to the stability of the ACL. If these muscles aren't as strong, or don't activate as quickly, more strain is put on the ACL.
